


SARS-CoV-2 Origins: Potential Epidemiological Clues for Discerning Between a Disease Outbreak of Natural Origin Versus an Act of Bioterrorism
Analysis of the unusual SARS-CoV-2 outbreak showed that natural origin is questionable and suggested it was a consequence of an accidental laboratory release.

It was recently reported that World Health Organization (WHO) has abandoned plans for its second phase of scientific investigation into the origins of the COVID-19 pandemic. Given that scientists and officials in China have now had over three years to hide, destroy, and/or falsify any evidence we may never know for certain where SARS-CoV-2 originated.
“There is no phase two,” Maria Van Kerkhove, an epidemiologist at the WHO in Geneva, Switzerland, told Nature. The WHO planned for work to be done in phases, she said, but “that plan has changed”. “The politics across the world of this really hampered progress on understanding the origins,” she said.
Discerning Between Natural and Intentional Disease Outbreaks
When a suspicious disease event occurs, it can be difficult to determine if it was caused by nature, an accident, sabotage, or an act of biological warfare or terrorism. This has been the case with the SARS-CoV-2 pandemic. Three years after the pandemic was declared and it is still unknown as to whether this virus originated from nature or was released from a research laboratory, whether intentionally or by accident. The question remains as to whether or not SARS-CoV-2 was deliberately released as a biological weapon.
Epidemiological Tools for Discerning a Deliberate Epidemic
There are three epidemiological methods for differentiating between an outbreak by natural causes and a potential biological weapons release.
Grunow & Finke developed an epidemiological assessment tool to identify or rule out a biological warfare agent in the event of an unusual infectious disease outbreak using qualitative assessment criteria. This evaluation scheme described two types of evaluation criteria: conclusive and non-conclusive. Conclusive criteria include the proven identification of the cause of illness as a biological warfare agent, or proof of the release of an agent as a biological weapon. With non-conclusive criteria, the greatest significance (assignment of higher weighting factors) is credited to the existence of a biological threat or risk, special aspects of a biological agent, a high concentration of biological agent in the environment, and epidemic characteristics.
Table 1. Non-conclusive criteria for assessing an epidemic in order to rule out the use of a biological warfare agent
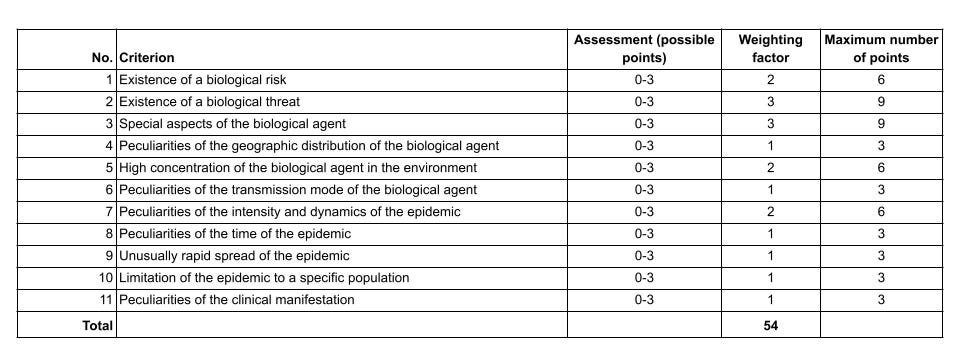
Each criterion is assigned a value on a scale of 0-3, depending on the data collected in the study of the source of infection, on the analysis of the politico-military, social and ecological situation and on intelligence information gathered. The non-conclusive criteria are also weighted according to their usefulness for assessing the possible use of a biological warfare agent. For this purpose, a multiplication factor (weighting factor) is used which has been determined on the basis of the operational, medical and epidemiologic significance of the individual characteristic:
1—Criterion can also be explained by natural causes (non-weighted criterion).
2—Criterion can be explained by natural causes only to a limited extent or under special circumstances, or arouses the suspicion that a biological warfare agent has been used (weighted by a factor of 2).
3—Criterion cannot be explained either fully or at all by natural causes, or indicates the likelihood of the use of a biological warfare agent (weighted by a factor of 3).
The likelihood that an epidemic has an artificial cause can be determined by non-conclusive and conclusive criteria. This is done by first determining the total number of points while taking into consideration the assessment and weighting of the various non-conclusive criteria (Table 1). The number of points is then compared with an arbitrary scale of probability and then assessed: unlikely (0–33% confidence)=0–17 points; doubtful (18–35% confidence)=18–35 points; likely (67–94% confidence)=36–50 points; highly likely (95–100% confidence)=51–54 points.
In 2006 Dembek, et. al. developed an epidemiological assessment tool to identify or rule out release of a biological warfare agent in the event of an unusual infectious disease outbreak, using specific criteria. Eleven potential epidemiological clues are provided to for discerning between a deliberate release of a infectious disease and a natural outbreak that may mimic an act of bioterrorism.
Clue no. 1 – A highly unusual event with large numbers of casualties. Naturally spread illness may cause a large group of ill individuals.
Clue no. 2 – Higher morbidity or mortality than is expected. A higher morbidity or mortality than typically observed for a particular disease may provide a clue to an unusual event.
Clue no. 3 – Uncommon disease. Many infectious diseases have predictable distributions based on environmental, host, and vector factors.
Clue no. 4 – Point-source outbreak. In an intentional event, dates of onset would probably depict a point-source outbreak curve.
Clue no. 5 – Multiple epidemics. Multiple perpetrators in collaboration could release a single biological agent at various locations, or even multiple agents from multiple locations.
Clue no. 6 – Lower attack rates in protected individuals. This clue applies to military populations, and also to those in buildings with filtered air supply.
Clue no. 7 – Dead animals. Animals have been used historically as sentinels of human disease.
Clue no. 8 – Reverse spread. The typical pattern with a zoonosis is disease occurring in a susceptible animal population, being followed by cases in humans.
Clue no. 9 – Unusual disease manifestation.
Clue no. 10 – Downwind plume pattern. It is useful to plot locations where cases occur on a geographic grid or map.
Clue no. 11 – Direct evidence. A perpetrator leaving evidence would make determining the intentional cause of illnesses easier.
These clues are dependent upon public health authorities and their capacity for disease surveillance, laboratory, and outbreak investigation and assessment using these clues is subjective.
The Radosavljevic–Belojevic method has two parts. The first part for early orientation and differentiation of unusual epidemiological events (UEEs) and it uses eight qualitative and six quantitative indicators.
Table 2. Scoring of the COVID-19 outbreak according to the model of Radosavljevic and Belojevic [7,9] for differentiation between natural, accidental, and deliberate outbreak caused by new or re-emerging pathogen.

The second part of the method is subtle and detailed differentiation of the four possible UEE scenarios: natural outbreak of a known disease, natural outbreak of a new or re-emerging disease, outbreak by an accidental release of a pathogen, and outbreak by a deliberate delivery of a biological agent. A total of 47 indicators are used in this method. In both parts of the method, indicators are scored with 1 if they were present in the outbreak, and scored with 0 if indicators were not present in the outbreak.
Case Review of SARS-CoV-2 Pandemic
While we may not find definitive evidence as to the origins of SARS-CoV-2, an epidemiological assessment tool can be applied to this outbreak that may help public health authorities determine if SARS-CoV-2 was deliberately used to initiate the pandemic.
Analysis was performed according to the Radosavljevic–Belojevic method for outbreak scoring and differentiation. The two other methods for outbreak differentiating were deemed not appropriate for the COVID-19 outbreak. They focus on differentiating between natural and deliberate outbreaks and do not have scenarios for accidental outbreaks and outbreaks caused by a new or re-emerging pathogen.
Based on this method, the total score for part 1 (Table 2 above) was 13 out of 14 points, which meant it was probably an artificial (deliberate or accidental) outbreak.
Assessment of the COVID-19 pandemic origin in 2019–2020 by differentiation scoring for a natural outbreak of a disease (NE), a natural outbreak of a new or re-emerging disease (NR), an outbreak by an accidental release of a pathogen (AR), and a deliberate outbreak (DO) scored 17 out of 33 points for AR (see Table 2 of the published article). This indicated an accidental release of a SARS-CoV-2 virus from the Wuhan Institute of Virology (WIV) was highly probable to be the cause of COVID-19 outbreak.
CONCLUSION:
In conclusion, this study suggests that the COVID-19 outbreak was a consequence of an accidental release of a new COVID-19 virus, probably during the technical accident and/or negligent violation of hygienic norms in the laboratory facility.
The presence of SARS-CoV-2 has not been detected through sampling and testing of bats more than 80,000 wildlife, livestock and poultry samples collected from 31 provinces in China. Therefore, an animal host has not be determined in more than three years since the outbreak was identified in Wuhan, China. We know without a doubt the laboratory at WIV was working with coronaviruses. Researchers were manipulating the virus via reverse genetics and through serial passaging in animal models. It is time to accept that SARS-CoV-2 originated at WIV, whether it was due to ill research staff, infected animals sold to the animal market or due to a faulty air handling system.

What about genome sequence signatures such as the furin cut site? If there were an intermediate host, seems that it would be infected and could be found. It is interesting that it has been detected in the deer population now among many other animals. So it now has a new animal reservoir. Exploring the animal reservoir around Wuhan it might be too late to find the original strain origins now as presumably the animals can be infected with the latest strain. If it was not a lab leak, then the government should have made it easy to investigate and confirm there was no leak-instead it has been blocked and China says a lab leak theory is all politics...
Thanks for this interesting article about pandemic assessment.