


The COVID-19 Pandemic Created A Perfect Health Storm
Another reason Americans fared worse during the pandemic was the high rate of obesity and malnutrition. Lockdowns exacerbated the issue since people gained more weight while staying at home.

Several independent studies have observed that people with obesity are at a greater risk of severe disease and death due to COVID-19.
Obesity is the Real Killer
While more than 75% of the COVID-19 deaths have been reported in people aged 65 years or above, risk factors for severe disease and death included obesity, hypertension, and type 2 diabetes.
A retrospective study from France showed a high prevalence of obesity (75.8%) in SARS-CoV-2 patients admitted to the ICU, as well as, those requiring invasive mechanical ventilation.
A body mass index (BMI) over 25 is considered overweight, and over 30 is obese. High body mass index (BMI) has particularly been found to be a strong indicator of disease severity in patients younger than 60 years of age. In fact, younger patients (Age < 60 years) with a BMI > 30 kg/m2 were more than twice as likely to be admitted to hospital and develop critical illness compared to patients with a BMI < 30 kg/m2. The likelihood of admission to ICU increased to 3.6 times in patients with severe obesity (BMI ≥ 35 kg/m2). Research is showing that people with a BMI of 35 to 40, risk of death from COVID-19 increases by 40% and with a BMI over 40 by 90%, compared to those not living with obesity.
The U.S. has a High Rate of Obesity
In the U.S., obesity rates have been steadily climbing for the past two decades. According to 2017–2018 data, over 40 percent of Americans are considered obese, 35 percent of whom are children aged 5 to 17. In addition, over 9 percent were within the severely obese threshold. As of this year, the U.S. has the 12th highest obesity rate in the world at 36.2%.

Source: https://www.statista.com/chart/20981/obesity-rates-on-the-rise-in-us/
What Makes the Obese so Vulnerable?
Obesity provides a unique microenvironment for disease pathogenesis, resulting in increased severity of disease and poor outcome. People with obesity have an increased prevalence of other chronic diseases like renal insufficiency, cardiovascular diseases, type 2 diabetes, certain types of cancers, and a significant degree of endothelial dysfunction.
The ultimate result of obesity is a state of chronic inflammation both at local as well at the systemic level.
Obesity is associated with significant alteration and abundance of immune cells in the adipose tissues with a marked decrease in Th2 cells, Treg cells, and M-2 macrophages (figure below). There is a significant increase in the abundance of pro-inflammatory cells like CD8+ T cells and M-1 macrophages. Obese, inflamed adipose can be comprised of greater than 40% M-1 macrophages, which are the source of an array of pro-inflammatory cytokines leading to a local as well as systemic inflammation. Several other cell types like neutrophils, dendritic cells, and mast cells also contribute to inflammation by releasing several pro-inflammatory factors.

Source: Figure 1. Dysregulated fatty acid metabolism, cellular hypertrophy and death, ER stress, Hypoxia and mitochondrial dysfunction, because of excess fat leads to a substantial alteration of cellular architecture of adipose tissue. This rearrangement favors a pro-inflammatory environment and perpetuates local as well as systemic inflammation. https://immunityageing.biomedcentral.com/articles/10.1186/s12979-020-00212-x
Given that COVID-19 as a disease is immune dysregulation which causes significant lung inflammation as well as inflammation in other organs, it is plausible to suggest that acute inflammation arising from COVID-19 may amplify existing chronic inflammation secondary to obesity and lead to more severe disease phenotype and poorer outcomes. In addition, chronic inflammation due to obesity not only leads to the premature aging of the immune system but also results in decreased responsiveness to infectious agents.

Source: Figure 2. Factors responsible for disease severity and poor outcome in obese COVID-19 patients. Obesity-associate chronic inflammation, impaired Immune function and increased ACE2 expression results in an increased disease severity and worse clinical outcome in obese subjects with COVID-19 infection https://immunityageing.biomedcentral.com/articles/10.1186/s12979-020-00212-x
Shutdowns and Lockdowns Exacerbated the Problem
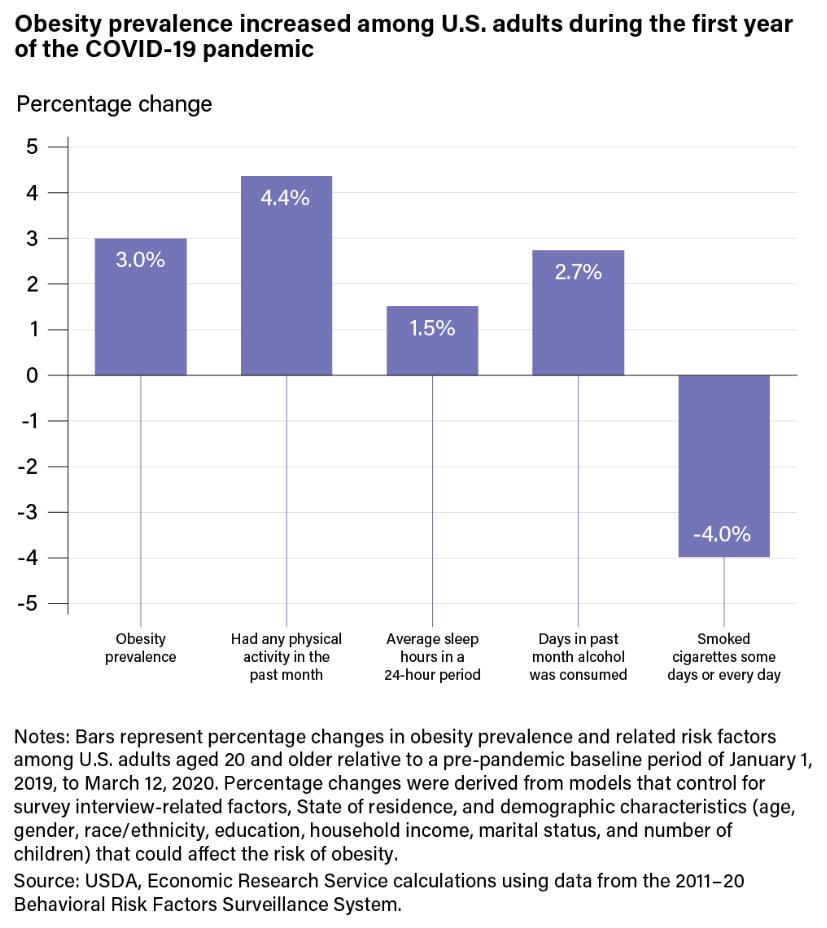
Most concerning is that adult obesity prevalence increased in the first year of the pandemic. Stress, gym closures, the desire for comfort food and being in close proximity to snacks when working from home all played a role in weight gain.
One study found that, compared with a pre-pandemic baseline period (January 1, 2019, to March 12, 2020), adult obesity prevalence was three percent higher over the period from March 13, 2020, to March 18, 2021, the first year of the COVID-19 pandemic.
Source: https://www.ers.usda.gov/amber-waves/2022/july/adult-obesity-prevalence-increased-during-the-first-year-of-the-covid-19-pandemic/#:~:text=The%20study%20found%20that%2C%20compared,of%20the%20COVID%2D19%20pandemic
Findings also showed statistically significant changes in each of the four obesity-related behaviors during the COVID-19 pandemic. Participation in exercise rose 4.4 percent, and people slept 1.5 percent longer. Meanwhile, the number of days in the period of a month in which alcohol was consumed was 2.7 percent higher, and cigarette smoking dropped by 4 percent. Research shows that increased use of alcohol and reduced cigarette smoking can lead to obesity and therefore may have contributed to the higher rates of obesity among U.S. adults during the pandemic.
Another study of over 3,400 participants found almost half of the respondents (48%) reported gaining some weight (≥10 pounds for 11% and ≤9.9 pounds for 37%) during the pandemic. The survey also found that those who reported being very overweight before the pandemic were the group most likely to gain weight (65%). Individuals who were obese or overweight had the highest prevalence of self-reported weight gain during the pandemic (56% and 54%, respectively).
Based on the findings of this and earlier studies, it seems like weight gain was higher among certain groups who were already vulnerable to poorer health outcomes (e.g., overweight before the pandemic and gained additional weight, higher stressors/deprivation before the pandemic, and greater prevalence of psychological distress during the pandemic, unhealthy diet and lower physical activity before the pandemic with worsening of diet and physical activity during the pandemic).
If the policies implemented had really been about health, public health professionals should have considered the indirect health effects of the pandemic policies beyond mitigating the effects of the virus. The fiscal and social policies implemented during the pandemic should have considered opportunities for increasing healthier diets and food security, physical activity and exercise in communities, mental health services and access to care, engagement in wellness programs, and preventive health screenings.
Unfortunately, due to the public health policies that were implemented, the psychosocial impact of the COVID-19 pandemic is likely to continue to impact body weight measures resulting in long-term burdens of chronic diseases and escalating healthcare expenses.