
The Herd Immunity Fallacy: Limits, Assumptions, and Reality
Why assumptions about population immunity don’t always hold

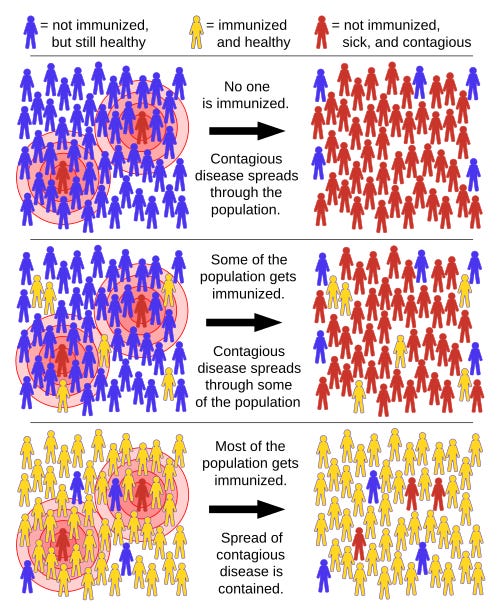
During the pandemic and in the wake of recent measles outbreaks, many have pointed to the concept of “herd immunity” as a key reason to get vaccinated. This cartoon highlights how herd immunity is sometimes oversimplified or misapplied in discussions about vaccination.

🐑What Is Herd Immunity?
When you think of a herd, you probably think of cows, wildebeest or buffalo. In the animal world, there is safety in numbers – more pairs of eyes to look out for predators, for example.
As humans, we don't generally have to worry about predators, but we can gain the protection of the herd in other ways.
Herd immunity — also called population or community immunity — means that enough people in a group or area have immunity to a germ (for instance, a virus) that it no longer spreads easily. That includes people who haven't caught the disease, people who had the illness and recovered, and people who got a vaccine.
📜History of Herd Immunity
Herd immunity didn’t start as a vaccination concept—it came from livestock science in the 1800s.
The term herd immunity was first used in 1894 by Daniel Elmer Salmon, Chief of the Bureau of Animal Industry (BIA), to describe the health and disease resistance of well-fed hog populations. The use of the phrase expanded in 1916 when BIA veterinary scientists used the term to describe immunity in cattle following infection with Brucellosis also known as “contagious abortion”—epidemics of spontaneous miscarriage—in cattle and sheep.
In 1923, British bacteriologists began using the concept in experiments involving epidemics in mice, as part of efforts to better understand patterns of disease transmission in human populations. Unless there was a steady influx of susceptible mice (this is an important to remember), the rising prevalence of immune individuals would end an epidemic. In a 1923 article in the Journal of Hygiene, Topley and G. S. Wilson described this phenomenon as “herd immunity”.
The idea moved into medicine and by the late 1920s, the concept had gained broader traction—particularly among British scientists—who used it to describe the accumulation of population-level immunity to diseases such as diphtheria, scarlet fever, and influenza. In 1922, Topley suggested a parallel between outbreaks in mice and children:
“Such a likeness would seem to exist in the case of epidemic diseases affecting children of school age.” He also wondered whether measures already “in vogue in dealing with epidemics among live-stock, where methods of segregation are so much more easily enforced than among human populations”, might inform decisions about school closings amid epidemics.
In a 1924 article in The Lancet, Dudley applied “herd immunity” to humans. In a 1929 article, “Human Adaptation to the Parasitic Environment”, he wrote,
“I will now consider the community, or the herd…Nations may be divided into urban or rural herds. Or we can contrast the shoregoing herd with the sailor herd, or herds dwelling in hospitals can be compared with those who live in mental hospitals.”
The concept of “herd immunity” became a fixture of epidemiology by the 1930s but the early researchers never settled on a clear definition.
Herd immunity took on fresh prominence in the 1950s and 1960s as new vaccines raised crucial questions for public health policy. The idea shifted from simply describing natural immunity to actively achieving population protection through vaccination. Mass vaccination, discussions of disease eradication, and cost–benefit analyses of vaccination subsequently prompted more widespread use of the term "herd immunity".
🔎Outlook for Achieving Herd Immunity
Herd immunity often results from a combination of people getting vaccinated and people getting infected with the microorganism (natural immunity). Both natural and vaccine immunity cause your body to make antibodies and immune cells that recognize a specific pathogen. Your body can then fight the pathogen off more easily the next time it sees it. It usually takes a large percentage of people with immunity to achieve herd immunity.
Source: https://en.wikipedia.org/wiki/Herd_immunity
This graphic oversimplifies herd immunity by not accounting for individuals who have already recovered from infection and developed natural immunity.
Public health discussions often emphasize vaccination because it can increase immunity without requiring large numbers of people to become ill at the same time.
Proponents of vaccines believe without vaccination, immunity would build more gradually through infection, which can allow ongoing transmission and lead to higher levels of illness and complications. For this reason, the concept of herd immunity is more complex than simple visual models suggest and depends on timing, population dynamics, and the characteristics of the disease itself.
It’s also important to recognize that herd immunity is not permanent. In a globally connected world, unless a disease no longer exists anywhere in the world, it can start spreading again. This can occur through travel or migration when individuals without immunity encounter populations with gaps in protection.
Therefore, herd immunity can only work in a closed system. Unfortunately, we don’t live in a closed system. As new babies are born without immunity and are being added to the susceptible pool of individuals once their maternal immunity wears off and people visit from outside the community who may reintroduce disease, outbreaks will occur.
Challenges in Reaching Herd Immunity
Herd immunity isn’t possible with every infectious disease. The idea of herd immunity may work for some diseases, such as measles. It was noted in 1933 that a measles outbreak in a community could be prevented if about 68% of children were already infected. Current estimates suggest that roughly 94% population immunity is required to achieve effective protection against Measles. That means 94 people out of 100 in a population need to be immune to stop the spread of the measles virus. That includes measles recovery or people who got both measles vaccine shots.
But it’s a harder concept to apply to illnesses like COVID-19.
Some reasons herd immunity might not be possible for certain diseases include:
The pathogen changes (mutates) frequently: This means you can get immunity to one version, but that may not protect you from a newer variant. There can also be multiple different versions of a pathogen that circulate at one time (like influenza). Herd immunity itself acts as an evolutionary pressure on pathogens, influencing viral evolution by encouraging the production of novel strains, referred to as escape mutants, that are able to evade herd immunity and infect previously immune individuals.
Immunity to the pathogen doesn’t last long enough: Immunity has to last a long time to prevent spread. For example, immunity from both infection and vaccination for some viruses lasts only a few months. A portion of those vaccinated may not develop long-term immunity. This usually isn’t long enough to achieve herd immunity.
The pathogen can spread when you have no symptoms: Microorganisms spread more easily when people don’t know they’re infected. This makes it much less likely to get herd immunity without vaccination.
The pathogen is found in nature: Herd immunity only works for diseases that spread from person-to-person. Some pathogens naturally live in soil or water (think tetanus bacteria or infectious fungi). Vaccines can protect you personally from some of these infections, but population immunity can’t be achieved.
Influenza, RSV and SARS-CoV-2 are all viruses that we might not be able to get herd immunity to because they mutate too often, they spread without symptoms or immunity doesn’t last very long (or a combination of these). Tetanus shots, on the other hand, last a long time. But we can’t reach herd immunity because the bacteria live in the environment, not exclusively in people.
The Myth of Herd Immunity for COVID-19
During the COVID-19 pandemic, scientists initially estimated that 60 to 80 percent of the population would need to acquire resistance to SARS-CoV-2 through vaccination or naturally acquired immunity to banish it.
Dr. Anthony Fauci frequently discussed herd immunity as a potential endpoint, initially suggesting that a significant portion (75 percent to 80 percent) of the population would need immunity to slow the spread of SARS-CoV-2. In broader public health messaging, herd immunity was also often cited as part of the rationale for policies aimed at increasing vaccination coverage, including mandates.
“Let’s say we get 75 percent, 80 percent of the population vaccinated,” Fauci said. “If we do that, if we do it efficiently enough over the second quarter of 2021, by the time we get to the end of the summer, i.e., the third quarter, we may actually have enough herd immunity protecting our society that as we get to the end of 2021, we can approach very much some degree of normality that is close to where we were before.”
However, for a vaccine to generate herd immunity, it must protect against infection with the virus in addition to preventing illness to significantly reduce the spread of the pathogen in the population. A vaccine that does NOT protect against infection and transmission of a pathogen cannot confer herd immunity.
The Vaccines textbook (Plotkin, 2013 6th edition) explains: If a vaccine were to protect only against disease, and not at all against infection, then it would have no influence on infection transmission in the community and there would be no indirect protection (vaccination of one person would have no influence on any others in the community). It would be possible to reduce disease with such a vaccine but not to eradicate the infection.
In other words, vaccines that do not prevent infection with the pathogen can never confer herd immunity.
It became evident early in 2021 as “breakthrough cases” were being reported, the COVID shots were not preventing infection with SARS-CoV-2. A total of 10,262 SARS-CoV-2 vaccine “breakthrough infections” had been reported from 46 US states and territories as of April 30, 2021. Beginning May 1, 2021, CDC transitioned from monitoring all reported COVID-19 vaccine breakthrough infections to investigating only those among patients who are hospitalized or died.
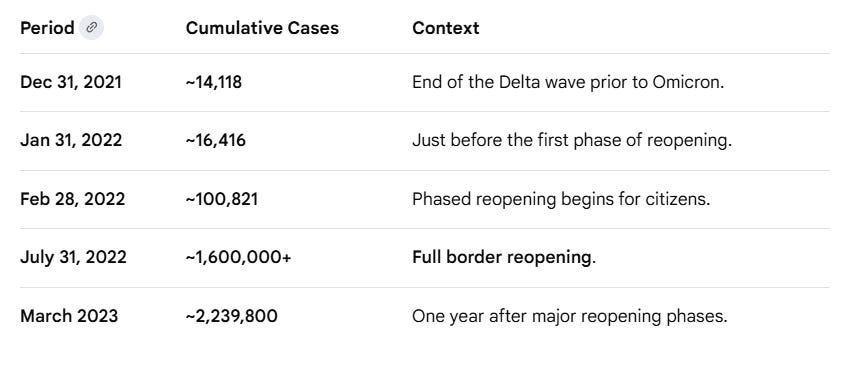
Another illustrative example is New Zealand. In March 2020, the country closed its borders to nearly all non-residents and pursued an “elimination” strategy for COVID-19. To transition out of strict lockdowns and ease border restrictions, officials later set a target of 90% full vaccination among the eligible population (aged 12+) within each District Health Board.
By mid-November 2021, New Zealand had reached approximately 90% first-dose coverage and about 80% second-dose coverage nationwide. A phased reopening followed, prioritizing citizens and skilled workers before fully reopening to international visitors in July 2022.
Because of its prolonged border controls and low case numbers, fewer than 1% of New Zealand’s population had been infected prior to reopening. This created a unique situation in which much of the population had little to no infection-acquired immunity, meaning population-level protection relied primarily on vaccination at the time borders reopened. Following reopening in early 2022, recorded cases rose sharply, reflecting a rapid increase in transmission.
Source: https://en.wikipedia.org/wiki/COVID-19_pandemic_in_New_Zealand

The rise in cases was primarily due to the highly contagious Omicron variant, which arrived in late December 2021 and became dominant as borders opened to more travelers. This example highlights how, even in a highly vaccinated population, changes in viral dynamics and population immunity can significantly influence transmission patterns, underscoring the challenges of achieving and maintaining herd immunity in a real-world, globally connected setting.
mRNA “Vaccines” Were not Designed to Achieve Herd Immunity
In the clinical trial of the Moderna COVID-19 mRNA injection, the main outcome measured was prevention of symptomatic COVID-19 rather than prevention of infection and transmission.
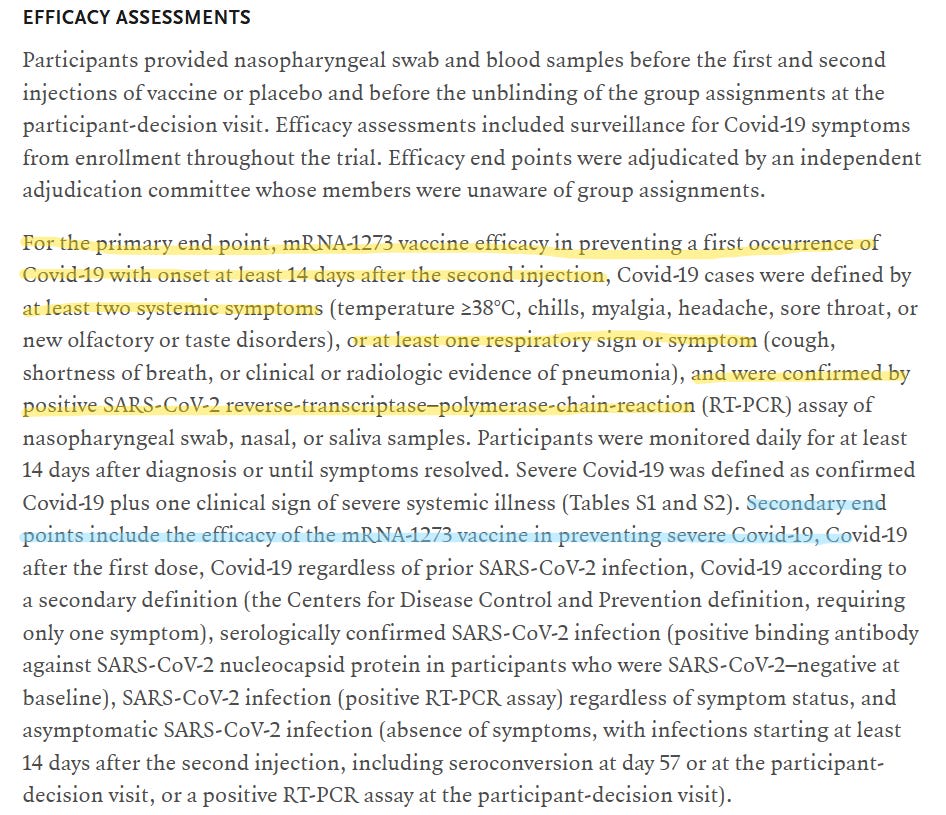
The clinical trial endpoints described in New England Journal of Medicine for the Pfizer-BioNTech BNT162b2 COVID-19 mRNA shot also focused primarily on preventing symptomatic COVID-19, rather than directly measuring transmission.
A Pfizer executive later confirmed that the company did not test whether the vaccine stopped transmission (spreading the virus to others) before it was released to the public.

Given the highly mutable nature of SARS-CoV-2 and the fact that available mRNA vaccines (such as Pfizer-BioNTech COVID-19 Vaccine and Moderna COVID-19 Vaccine) were primarily designed to reduce symptomatic illness rather than fully prevent infection, achieving classical herd immunity became increasingly unlikely in the traditional sense. In practice, even very high levels of vaccination would not necessarily stop transmission entirely, particularly with the emergence of more transmissible variants and waning immunity over time.
CONCLUSIONS:
During the COVID-19 pandemic, Herd Immunity became widely discussed—and often misunderstood. Factors such as waning immunity, viral mutation, and uneven vaccination rates highlighted that herd immunity is not a fixed threshold but a dynamic and context-dependent phenomenon.
Achieving herd immunity through vaccination depends on the ability of a vaccine to reduce both disease and transmission of the pathogen it targets. However, even vaccines that provide strong protection against illness do not necessarily eliminate infection or spread, particularly in the context of rapidly evolving viruses such as SARS-CoV-2.
Even under idealized assumptions of highly effective or “sterilizing” immunity, maintaining herd immunity in practice is complicated by continual population turnover (birth of susceptible individuals), global migration, and the ease of international travel, all of which allow for repeated reintroduction of pathogens into communities.
As a result, herd immunity is better understood not as a permanent endpoint, but as a shifting balance influenced by biological, demographic, and global connectivity factors.
Del Bigtree measles, they never had herd immunity never will, only natural immunity is lifelong, injection immunity wanes in everyone.
https://t.me/delbigtree/134 ➡️🔴➡️